• Most medical bankruptcies were filed by people who had health insurance when their illnesses began.
• Nearly 40 percent of debtors who had a “major medical bankruptcy” had lost their insurance during the two years before filing, compared with 27 percent of filers citing no medical cause. In other words, loss of insurance is a primary path to bankruptcy.
• About 61 percent of those suffering a major medical bankruptcy went without needed doctor or dentist visits and about half failed to fill prescriptions. Both figures are significantly higher than those of respondents whose bankruptcies arose from non-medical causes.
Plainly, more than an insurance problem is at work here. Covered or not, if someone is too sick to work, he or she may lose paychecks and quickly sink into debt. And medical causes can include such behavioral issues as alcoholism and drug abuse.
Still, insurance is a key component. If you don’t have it, personal debt will rise even more quickly. What is more, illnesses that reduce the ability to work can result in loss of coverage and, with it, the ability to regain health, return to work and stanch the rising threat of financial ruin. Such is the internal contradiction of employer-provided health insurance.
Moreover, the survey results clearly show that it is not merely the lack of insurance that is a problem, but the insufficiency of insurance for those who have it. When Americans run into medical crises, their insurance may not be there for the long haul.
Elaine responded thus:
I will say that the numbers in this article don’t really match what I see in my practice. Mine are more depressing. I see far more people than this article indicates who have never had health insurance. In most cases, their employers don’t offer it. In some cases their employer offers it, but the employee’s share of the premium would be 40% or more of the employee’s gross income.
Part of it is Oklahoma; we live in a low-wage state. Part of it is the fact that employers have not had a lot of incentive to pay living wages as collective bargaining is very weak here (and, I suspect, across the country). And part of it is for the reasons that Michael Moore pointed out in his movie SiCKO.
Elaine says there are no easy answers. I disagree. It's not that the answers are not simple, it's that we don't have the will to implement them by public policy. We don't want to implement them because they will cost money (taxes that we will have to pay). But now the ounce of prevention has become the pound of cure. Health care dollars are now crowding out other important spending. (So are all the military entanglements the U.S. is engaging in around the world, but that is another topic.)
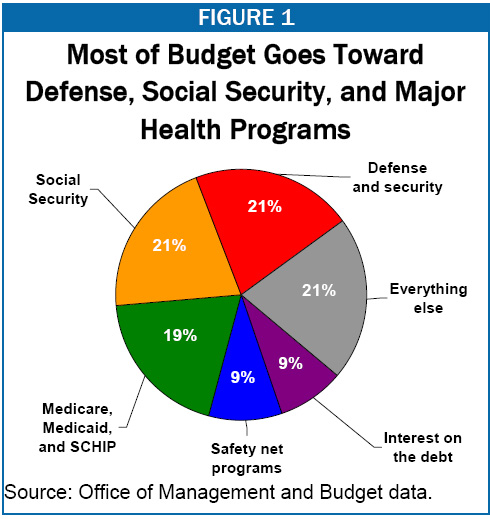
Image copied from the Center on Budget and Policy Priorities.
The neoconservative policy of Starve the Beast is also working in its perverse way. Our national debt is up to $6 trillion and the interest payments on the national debt equal almost 9% of our national budget. That may seem small, but that is just the interest. The national debt is currently equal to 38% of our Gross Domestic Product.
Deficit spending is nothing more than deferred taxation. The money that is borrowed to fund government spending today will have to be paid back somehow. Either taxes will have to be raised or the money supply will have to be inflated. We seem to be using the latter -- at least right now. But that also presents dangers due to the effect on America's financial stability around the world. At some point, the devaluation of our currency will lead Central Banks to start selling American dollars, further eroding confidence in our currency.
The ultimate point of all this is that it shows how our health care system is in serious condition and needs surgery -- and soon.
On its surface, it may seem like a national health care program would be too expensive to implement, but actually it's not. A national health care program would save money in the long term due to the implementation of the economy of scale. Furthermore, money recaptured due to no longer trying to turn a profit off of American's ill health would then be directed into productive areas. As long as the tax base was broadened to include those who are capable of paying (corporate, capital gains and estate taxes), it would be relatively painless to convert to a government-funded system. All we need is the political will.
1 comment:
Okie, love your blog!
Again, I disagree with your last paragraph.
The real reason national healthcare systems are able to lower costs are one simple fact: 4% of people use 70% of healthcare expenditure.
If anyone wants to 'cut costs', going after 70% is clearly the 'low hanging fruit'.
Many people seem to trust national healthcare system's rationing decisions more than they trust private system's decisions(though this is not universally true.. Switzerland and to some degree Germany come to mind).
Most people are not one of the 4% of patients who get rationed. And cutting these patients has a massive impact on healthcare spending. So as most people do not see/feel the pinch of rationing, but most people see lower costs, they like their nationalized systems/don't mind the rationing.
But Make no mistake, national healthcare systems work because they ration care and from my perspective, the real issue was really just trust.
In fact, there are some econophysicists who feel trust is the single largest predictor of a society's wealth.
And there is interesting research suggesting wealth inequality diminishes societal trust.
Yet there are models suggesting wealth inequality may be fundamental of evolutionary complex adaptive systems (notably Sugarscape).
I have no solution for these apparantly conflicting issues (if they are real in the first place).
But I do not agree with the current framework of the public vs. private healthcare debate. I see these as smokescreens for the bigger trust issue. And these are heavily influenced by the biology of morality.
A few Links:
1. Cuture is important/intertwined with trust.
2. Trust is intertwined with morality.
Post a Comment